
West Oncology APP Virtual: Updates in Lung Cancer Treatment with Dr Jason Porter
Presentation by Jason Porter, MD, West Cancer Center
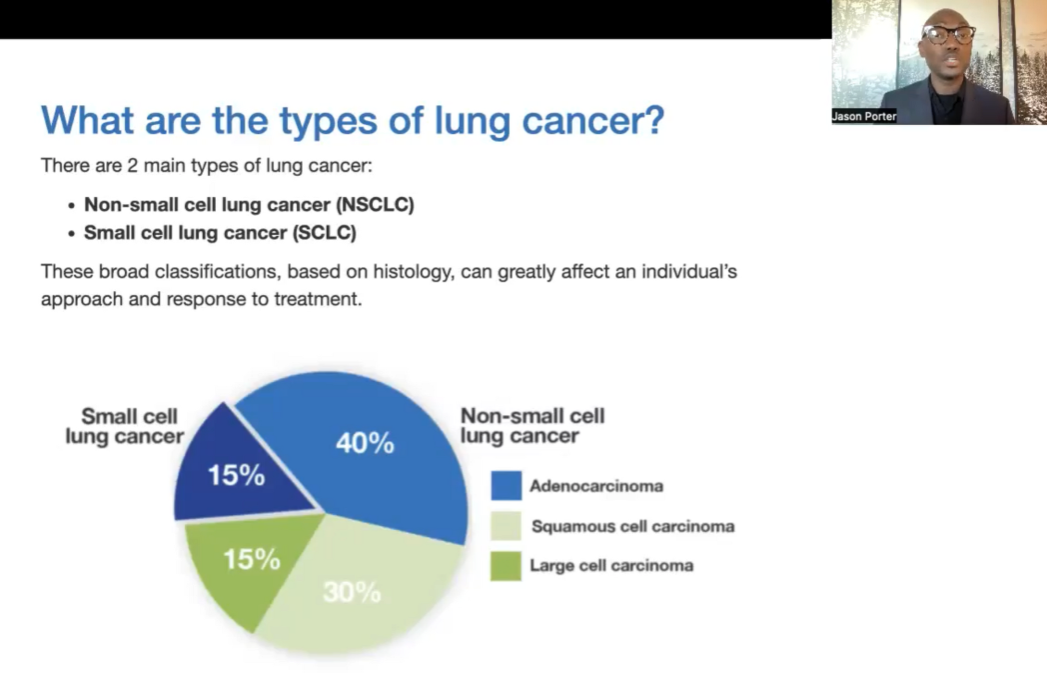
At the 2023 West Oncology Virtual Conference for Advanced Practicioners and Nurses presented by Total Health, Dr Jason Porter from West Cancer Center highlighted some of the recent updates in treatment for lung cancer. Dr Porter noted several key findings across clinical trials for patients with non-small cell lung cancer (NSCLC), the most common subtype of lung cancer, as well as the less common subtype of small cell lung cancer (SCLC).
Dr Porter noted that NSCLC can be further subdivided according to histologic subtype, with adenocarcinoma being most common (55%), squamous cell carcinoma constituting about 34%, and other subtypes, about 11%. Importantly, adenocarcinomas in NSCLC are now further distinguished according to specific molecular alterations, or mutations in the tumor’s DNA, which can be identified through the use of next generation sequencing (NGS) technologies on the biopsy sample. Some of the most common alterations include those occurring in the EGFR and KRAS genes. The identification of these and other molecular alterations, also known as ‘driver mutations’, allows for the use of targeted therapies, which can specifically inhibit the growth of that patient’s cancer, and often with a much lower toxicity, as compared to conventional chemotherapy. Immunotherapies, which allow the body’s immune system to more effectively recognize and kill cancer cells, are another essential component of the current lung cancer treatment paradigm.
Updates in Non-Small-Cell Lung Cancer
Osimertinib in EGFR-mutant (EGFRm) NSCLC
Dr Porter reviewed data from the phase III ADAURA Trial, which examined the use of an EGFR inhibitor, osimertinib, or placebo, as adjuvant (post-surgical) treatment for three years in patients with successfully resected NSCLC having an EGFR mutation (EGFRm). Early results from this trial showed a significant improvement in disease-free survival (DFS) for patients on osimertinib relative to placebo, with an overall 73% relative reduction in progression for patients on the active treatment at the most recent analysis. Central nervous system (CNS) metastases were also significantly reduced with osimertinib, and the benefit was observed in relevant subgroups of patients including those with stage IB, II, or IIIA disease, and regardless of whether they had received prior chemotherapy. Overall survival (OS) was also significantly improved for patients on osimertinib, and the results from ADAURA established osimertinib as the standard of care for patients with early stage, resectable EGFRm NSCLC. ADAURA was also the first phase III study to demonstrate a statistically significant and clinically meaningful OS benefit with an EGFR inhibitor in the adjuvant setting for lung cancer.
Immunotherapy with Checkpoint Inhibitors (ICI) + Chemotherapy
Dr Porter then reviewed treatment options for patients with EGFRm and progression while on osimertinib, or for those patients presenting with metastatic disease (stage IV) and progression on a prior EGFR inhibitor, noting the results from the KEYNOTE-789 Trial (NCT03515837). Patients in the trial had stage IV nonsquamous NSCLC, and were treated with either an immune checkpoint inhibitor (ICI), pembrolizumab, or placebo, in addition to a platinum doublet chemotherapy. The results showed a trend towards improvement in both progression free survival (PFS) and OS, however the benefit was minimal, and results for OS did not reach statistical significance. In this regard, Dr Porter noted that patients with resistance to EGFR inhibitors may have developed new molecular alterations, such as MET amplification, and these mechanisms need to be further studied to determine if they can be treated using other targeted therapies.
Neoadjuvant Immunotherapy + Chemotherapy
In the CheckMate 816 trial, the use of neoadjuvant (pre-operative) immunotherapy with nivolumab, in combination with chemotherapy, was compared with chemotherapy alone in early-stage NSCLC patients who were candidates for surgery and did not have driver mutations like EGFRm. In previously reported results from the trial, both event-free survival (EFS) and pathologic complete response (pCR) rates were significantly improved with the combination therapy versus chemotherapy alone. Dr Porter reviewed more recently reported exploratory results comparing outcomes for those patients who did, or did not receive definitive surgery following their neoadjuvant treatment. The results showed that more patients on the combination therapy were able to undergo definitive surgery, and both EFS and time to distant metastasis (TTDM) were improved with the combination versus chemotherapy alone. The results of the trial support the use of neoadjuvant nivolumab + chemotherapy as a standard treatment option for patients with resectable NSCLC.
In the KEYNOTE-671 trial, the use of neoadjuvant immunotherapy with pembrolizumab, in combination with platinum-based chemotherapy was compared with platinum-based chemotherapy alone for patients with early-stage NSCLC. Following neoadjuvant treatment, all patients underwent surgery, followed by adjuvant pembrolizumab or placebo. The results showed a significant EFS benefit of pembrolizumab over placebo, in the percentage of patients achieving a major pathologic response (mPR; 30.2% vs. 11.0%; P<0.00001), and in the percentage of those achieving a pCR (18.1% vs. 4.0%; P<0.00001), and the benefit of perioperative pembrolizumab was seen regardless of whether the patients achieved an mPR or a pCR. Results for OS have not reached statistical significance but continue to mature, and Dr Porter noted that approval of this treatment approach is awaited.
Updates in Small-Cell Lung Cancer
Treatment of Extensive Stage (ES) SCLC
Like NSCLC, for the rarer subtype of SCLC cancers, Dr Porter noted that SCLC subtypes such as ASCL-1, NEUROD1, and POU2F3 have been identified which have different biologic characteristics, although the clinical relevance of SCLC subtyping for treatment requires further study. The use of immunotherapy with an immune checkpoint inhibitor (ICI), in combination with platinum doublet chemotherapy (PDC) is the current standard treatment for SCLC, as evaluated in studies such as CASPIAN (durvalumab + PDC) and IMpower 133 (atezolizumab + PDC). Notably, the primary adverse event (AE) in these studies is myelosuppression, or a reduction in blood cell counts, which could lead to higher infection risks for patients on this therapy. Myelosuppression occurs primarily due to the suppression of hematopoietic progenitor cells in the bone marrow by the PDC, and in this regard, the use of trilaciclib, a cyclin-dependent kinase (CDK) 4/6 inhibitor, administered prior to EP therapy, has been shown to reduce myelosuppression. In one study, for example, the rate of grade 4 severe neutropenia (SN) was reduced from 42% to 5%, as was the need for supportive care measures such as blood cell transfusions, with the use of trilaciclib in addition to PDC. Following progression on either the CASPIAN or IMpower 133 regimens (which are the current standard of care for ES-SCLC), Dr Porter noted that lurbinectedin is an effective second line option, with an overall response rate (ORR) of 35.2% seen in one study.
Increasing Targeted Treatments in SCLC
With an increased understanding of the different SCLC subtypes, the potential for using more targeted therapies is growing. Tarlatamab is a bispecific T-cell engager (BiTE)-type therapy that is designed to bind the delta-like ligand 3 (DLL-3) molecule, which is expressed on ~85% of SCLC cells, and the CD3 receptor on T-cells of the immune system, resulting in T-cell mediated tumor lysis. In phase I studies (NCT03319940) tarlatamab has shown anti-tumor efficacy with manageable safety in patients with relapsed or refractory (R/R) SCLC. Tarlatamab is currently being compared with standard of care in a phase III study of patients with R/R SCLC that has progressed after at least 1 prior line of chemotherapy.
In a phase II study, the use of maintenance immunotherapy with atezolizumab was compared with atezolizumab in combination with talazoparib, a PARP inhibitor drug, for those patients having ES-SCLC with an SFLN 11 mutation (NCT04334941), with the primary endpoint of PFS. The results showed a trend toward improved PFS and OS with the addition of talazoparib to the regimen, but the results did not reach statistical significance. It is hoped that, with further study of tarlatamab and the atezolizumab + talazoparib combinations (targeting DLL-3 and SLFN-11, respectively) will expand the targeted therapy approaches for SCLC.
In the final portion of his presentation, Dr Porter described results for ifinatamab deruxtecan (I-Dxd) an antibody-drug conjugate (ADC) molecule directed against the B7-H3 antigen. Early studies with this agent (NCT04145622) in SCLC have shown the drug to be well-tolerated, with, what Dr Porter described as an “unprecedented” ORR of 52%, as well as a median duration of response of 5.9 months, a median PFS of 5.6 months, and a median OS of 12.2 months, in heavily pretreated SCLC patients. Notably, the rate of response was not impacted by the level of B7-H3 antigen expression. The drug is currently under investigation in a phase II study (Ideate-1; NCT05280470) of patients with ES-SCLC with 1 to 3 prior lines of therapy.
Quick Summary: Lung Cancer Updates with Dr Porter
Targeted therapy and immunotherapy continue to play an integral role for patients with early-stage NSCLC:
Osimertinib improves OS for early-stage EGFR mutation positive NSCLC.
Following progression on osimertinib, treatment with an immune checkpoint inhibitor, in combination with chemotherapy, remains sub-optimal approach.
Continued research is needed to identify molecular drivers of resistance to osimertinib.
Neoadjuvant immunotherapy with nivolumab + chemotherapy improves the key endpoints of EFS, TTDM, and EFS2 without increasing toxicity.
Perioperative immunotherapy with pembrolizumab + chemotherapy has been shown to improve EFS, and OS data continues to mature.
Immunotherapy approaches, second line treatment, and expanding targeted treatments for SCLC:
Immunotherapy with durvalumab or atezolizumab in combination with standard platinum doublet chemotherapy improves OS for patients with extensive stage (ES)-SCLC and represents current standard of care.
Lurbinectidin is an option for second line treatment following relapse on these regimens.
Trilaciclib is an effective treatment for chemotherapy-induced myelosuppression associated with these regimens.
Tarlatamab (targeting DLL-3) and the atezolizumab + talazoparib combination (targeting SLFN-11 mutation) show promise, and will hopefully usher in an era of more targeted approaches in SCLC.
Ifinatamab deruxtecan (I-Dxd) is in development for relapsed/refractory SCLC, with promising early results, and further studies underway.
Speaker Disclosure Information: Dr Porter reported no disclosures for this presentation.
Related Resources