
Artificial Intelligence: How Can it Enrich Cancer Care Access?
Presentation by Dr Arash Shaban-Nejad, PhD, MPH, University of Tennessee Health Science Center
At the Total Health 2023 ASCO Review held in Memphis, Tennessee, Dr Arash Shaban-Nejad from University of Tennessee Health Science Center presented on the topic of using artificial intelligence (AI) methodologies in cancer care as a means to increase access in the community setting, specifically in the West Tennessee area.
The Problem
Dr Shaban-Nejad began with an overview of leading causes of death in 2022, with heart disease and cancer as the top 2 respectively, followed by unintentional injury and COVID-19 as 3rd and 4th, noting that all of these can, at some level, be impacted by social, behavioral, economic, and environmental determinants of health, and that many of these determinants are modifiable. He provided examples of how factors such as insurance coverage and geographical location (i.e., lack of transportation) can lead to interruptions in cancer therapy, for example, radiotherapy, leading to poorer cancer outcomes. He noted that there have been few studies to evaluate what interventions can be done, at the health system level, to try and address these determinants of health, specifically to collect, integrate, and analyze individual and population level data, to develop interventions, and then to assess how effective the intervention may have been to correct the problem. Technologies like so called “precision medicine”, for example, not only require an understanding of how a person’s genes, or other “biomarkers” can impact a complex disease process like cancer, but also, what role do things like their environment and lifestyle choices play, and how do they interact with these factors. As such, understanding all of the complexities of a disease like cancer for the individual person, and then applying that understanding to the population in general, is a process that requires processing very large volumes of multidimensional data, and the use of AI is well suited to this process.
Dr Shaban-Nejad highlighted some of the long-term goals of precision medicine initiatives, for example, to create a vast database of over 1 million Americans willing to share their genetic information, clinical/biologic samples, and their diet/lifestyle choices, as well as their electronic medical records. To do so requires a new model for doing science that emphasizes engaged participants, responsible data sharing, and of course appropriate protections for patient privacy. The “data sharing” aspect is especially important in this regard as it requires sharing the same data across multiple applications and users. Applying AI interventions to the very large clinical problem of cancer is also complicated because a complex web of causality exists and a lot of data may be relevant, some of which may, or may not be attributable to a particular patient. Additional challenges may exist such as the heterogeneity of data sources (i.e., data coming from different sources), time and place of the data collection, and the data may or may not be representative of the population to be studied. One of the main functions of AI in this scenario, he noted, is to fuse all of this multidimensional data together across a single platform to generate meaningful information.
The Framework
Dr Shaban-Nejad described the AI project currently underway at his center, The ENRICH Project (Enriching Cancer Care Access in West TN), which is funded by the State of Tennessee Department of Health. The main purpose of ENRICH is to implement and validate X-CART, an AI-driven, automated informatics strategy that is designed to improve access to radiotherapy for vulnerable cancer patients, and reduce what he terms RTI, or radiotherapy interruption, with the use of a personalized, social support system. He noted that, essentially, the project is designed to identify patients who are at risk for RTI, and prioritize them for an appropriate intervention strategy. The hope is that the program will lead to better patient communication, improve the regional cancer support process, and most importantly, reduce the disparity in cancer outcomes for underserved populations. Some of the ways that what he calls “Health Intelligence” methods can be used to better understand, and ultimately improve population and individualized health are outlined in Box 1.
Box 1. Promise and Process: Transforming Population and Individualized Health with Health Intelligence
The Promise:
Using tools and methods from AI and data science, “Health Intelligence” aims to provide better insights, reduce waste and wait time, increase speed and service efficiency, accuracy, and productivity in health care and medicine.
The Process:
I) Integrate a very large volume of data
II) Conduct a statistical and quantitative analysis
III) Process structured and unstructured data to find patterns of interest
IV) Use these patterns of interest to come up with explanatory and predictive models
In the setting of healthcare, Dr Shaban-Nejad noted that it is especially important to use explainable AI, or XAI methods to improve fairness, accountability, transparency, and trust in healthcare. XAI differs from the more traditional AI and machine learning technologies, whereby the method the computer uses to come up with its conclusions is not known – essentially a “black box”. Instead, XAI provides an explanation of the methodology the computer used to derive its conclusion, and presents this method in an explainable interface with the user, so that the conclusions can be understood/checked/verified by the user, and are thus more reliable and trustworthy.
In the X-CART (eXplainable CAncer Radiation Therapy) platform, individual patient information from electronic health records, demographics, clinical data, as well as social determinants of health (SDoH) is collected and analyzed to produce what is known as a knowledge graph, which allows for new knowledge to be acquired through logical inference, and deep learning algorithms based on the graph which can classify the data, predict relationships, as well as engineer new features and metrics. The results are then validated by domain experts and any new facts/learnings are written back into the original knowledge graph to continue the learning process.
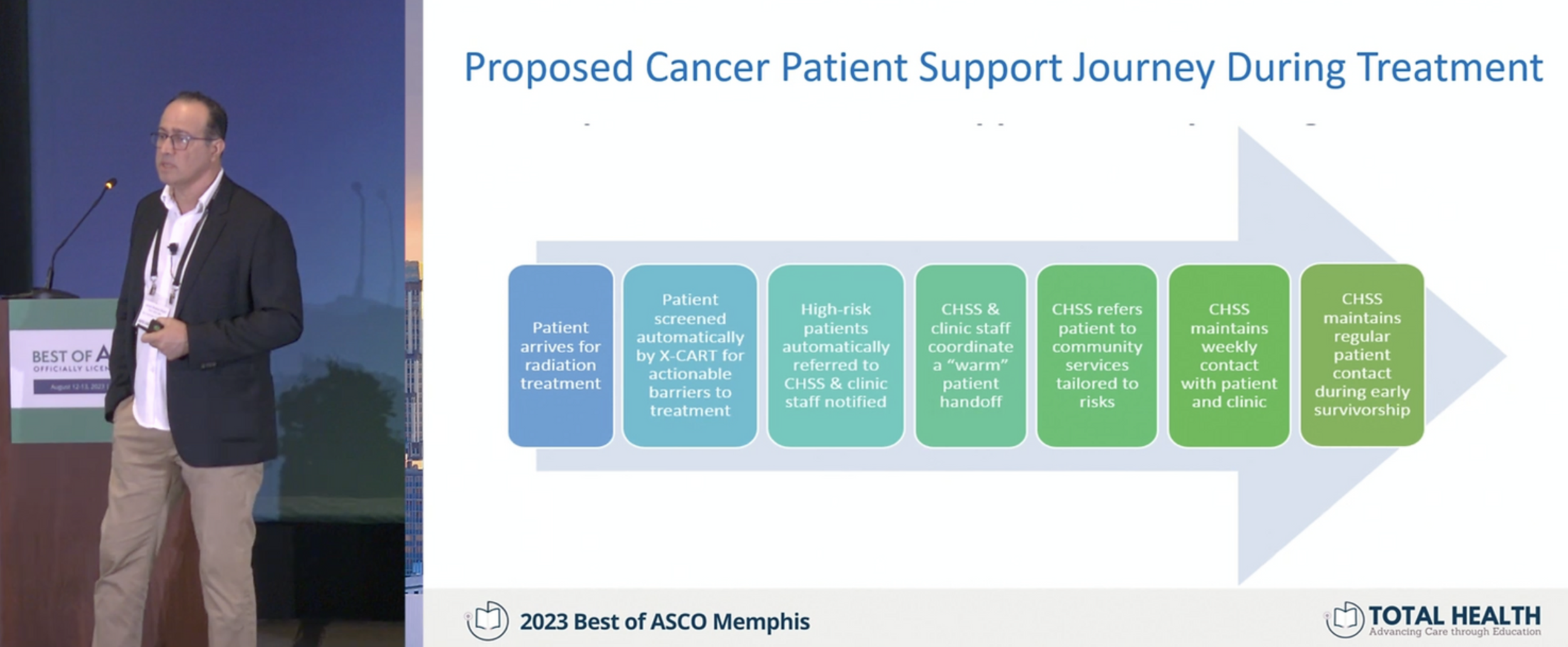
He explained the journey of a hypothetical radiotherapy patient through the X-CART system, whereby a new patient would automatically be screened for any barriers to completing their treatment, and any patients determined to be “high-risk” would be referred for appropriate supportive resources. For example, if SDoH are identified as an area of need for the patient, they would be referred to resources that could provide things like housing, food, childcare, legal or financial assistance, etc. In another example, if patient well-being is identified as an area of need, they would be referred to resources such as cancer community support groups, one-on-one counseling, and so on.
The overall goal of using XAI systems, Dr Shaban-Nejad noted, is to process knowledge from a large volume of data in order to provide causal explanations. Using this approach, Evidence Based Public Health (EBPH) strategies can be developed that encompass three types of knowledge and evidence with increasing complexity (Box 2), with the ultimate endpoint of determining how to implement the most useful interventions at the population level.
Box 2. Three Tiers of Knowledge in Evidence Based Public Health (EBPH)
Type I Knowledge (Simplest)
Examines causal relationships, associations, and correlations; what are the likely causes/contributing factors to the problem?
Type II Knowledge (More Advanced)
Examines the effectiveness of current interventions; what impact do they have on the problem?
Type III Knowledge (Most Advanced)
Based upon the specific population and needs, how can we best implement these interventions?
The System
In the final portion of his presentation, Dr Shaban-Nejad briefly outlined some of the current systems, including POPHR (Population Health Record) which allows the user to investigate a specific condition, for example diabetes, and its risk factors based upon real world data. Another system he described, MEMPHY-SYS, is a Metropolitan COVID-19 Data Registry that is linked directly to COVID-19 testing and used for population health surveillance. The dashboard in the MEMPHY-SYS system allows the user to read out daily positive cases and stratify by race (e.g., White versus Black), insurance coverage (yes or no), and a wide range of other parameters. An example of a correlation in this regard was that there was more frequent interruption of radiotherapy (RTI) at times of high COVID-19 infection (as would be expected); another factor that influenced RTI was patients living in geographic areas (defined by zip codes) that had lower socioeconomic status (SES). In so doing, causal relationships between “upstream” risk factors like SES can be linked to “downstream” health consequences (e.g., poorer cancer outcomes due to RTI).
Summary
Summarizing, Dr Shaban-Nejad outlined how the prospect of AI-enabled “precision oncology” or precision population health approaches can be used to enhance cancer care and access by supporting inferences about: 1) sources and motivation (i.e., “Who? Why? Where? When?” type questions, defining the problem), 2) characteristics of knowledge questions (i.e., “What? How?” type questions, defining the likely causes of the problem), and 3) consequence-type questions (i.e., how effective is a given intervention and/or what effect does it have on the problem). The promise of such technology is that it can reveal new knowledge, relationships and dependencies from already existing/available data sources; it is also both understandable by the user and verifiable (i.e., not just “blindly trusting the computer…”). Some of the challenges remaining in this area include legal issues, such as patient privacy, and ethical considerations (a “need to keep Humans in the loop” for the decision-making process).
Dr Shaban-Nejad is Associate Professor and Director of Population and Precision Health at University of Tennessee Health Science Center.
Speaker Disclosure Information: Dr Shaban-Nejad listed no disclosures for his presentation.
Related Resources