
Breast Cancer Susceptibility Germline Mutations: Genetic Testing and Management
Presentation by Dr Claudine Isaacs, Georgetown University
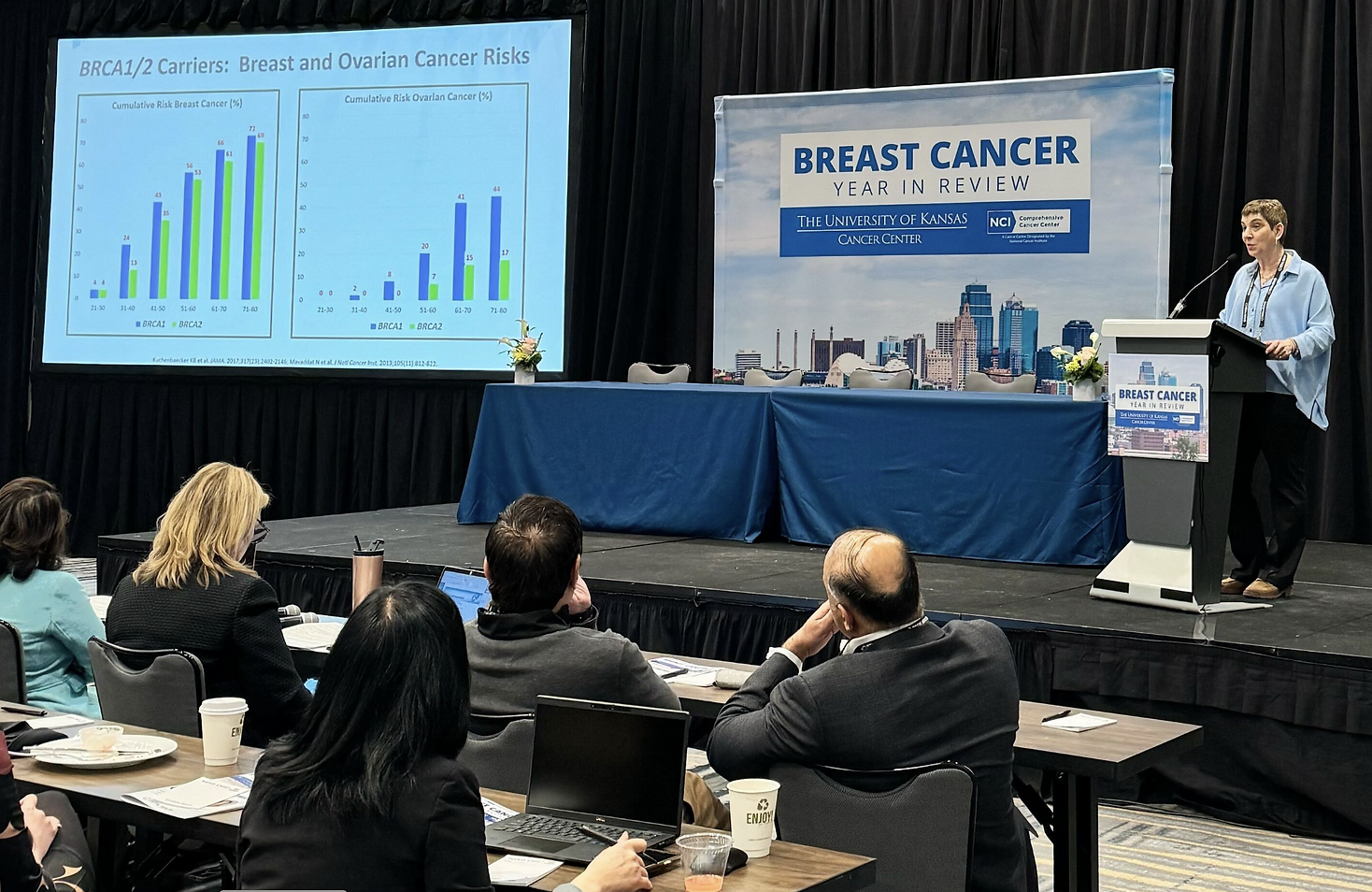
At the 2024 University of Kansas Breast Cancer Year in Review presented by Total Health, Dr Claudine Isaacs from Georgetown University presented on the topic of genetic testing in breast cancers, with a focus on the breast cancer susceptibility (BRCA) genes. We now know that certain patients who present with a diagnosis of breast cancer may have specific genetic alterations in their DNA, called germline mutations, which can cause them to have an increased familial risk for breast cancer, and these genetic alterations can have implications for their immediate relatives and/or children.
Genes Associated with Breast Cancer Risk
BRCA1 and BRCA2
The breast cancer associated genes BRCA1 and BRCA2 are highly penetrant, meaning that individuals having a mutation in one of these genes are very likely to develop breast cancer over their lifetime. For example, in the 51 to 60 year old age group, one study found that the cumulative risk of breast cancer for individuals having a BRCA1 or BRCA2 mutation was as high as 56%, and these same individuals also had a risk of developing ovarian cancer of up to 20%. For individuals having germline (gBRCA) 1 or 2 mutations, Dr Isaacs reviewed some general considerations for clinical risk management, which include earlier, and more frequent breast exams and mammography/breast MRI screening as compared to the general population, as well as prophylactic risk reduction measures such as bilateral mastectomy (removal of both breasts) and bilateral salpingo oophorectomy (surgical removal of both ovaries). In the latter case of prophylactic oophorectomy, Dr Isaacs noted the important issue of the procedure rendering patients menopausal in their thirties or forties, which can lead to significant quality of life and/or sexual function issues that need to be discussed with the patient. In gBRCA carriers who do not have a history of breast cancer, hormonal therapy is often used to help minimize these symptoms.
Other Mutations and Breast Cancer Risk
For individuals having a mutation in the PTEN gene, Dr Isaacs noted a large recent study showing a higher risk for female overall breast cancer (7.88-fold), ductal invasive breast cancer (7.55-fold), ductal carcinoma in situ (DCIS, 11.56-fold increased risk), as well as other cancers like ovarian, endometrial, colorectal and thyroid, and in many cases these cancers tended to occur at an earlier age as compared with the general population. Dr Isaacs also reviewed data from the BCAC and CARRIERS studies, which examined the impact of germline mutations for a number of breast cancer associated genes in both international (BCAC) and US (CARRIERS) populations, comparing individuals with breast cancer to unaffected controls. BOX 1 shows results from CARRIERS for breast cancer risk associated with the BRCA genes, as well as some of the more moderately penetrant genes, including ATM, CHEK2, and PALB2. Similar findings were observed in the BCAC study. Of note, this study also demonstrated that a number of genes that were previously thought to be associated with an increased risk of breast cancer, in fact were not. This included NBN, MUTYH, and BRIP1.
Box 1 – Lifetime Risk of Breast Cancer for Carriers of Pathogenic Mutations Versus General Population
| High Penetrance Genes | Moderate Penetrance Genes |
|---|---|
|
BRCA 1 – ~50% BRCA 2 – ~50% |
ATM – 20 – 25% CHEK2 – ~25% PALB2 – 32% |
In view of the impact of these more moderately penetrant genes, Dr Isaacs noted that efforts are underway to better individualize risk and management plans for mutations in breast cancer associated genes. One example is the Polygenic Risk Score, or PRS, which is a model that incorporates the impact of variants in a number of other lower risk genes to determine how they impact the overall breast cancer risk for patients with a given breast cancer associated mutation, and no previous family history of breast cancer. BOX 2 shows how the risk for developing breast cancer is impacted for patients in the ‘low risk’ PRS group (10th percentile), as compared to those in the high risk PRS group (90th percentile) for individuals with mutations in BRCA 1 and 2, ATM, CHEK2, and PALB2. While the overall risk remains high for BRCA 1/2 mutation carriers regardless of the PRS group, the risk was substantively diminished, and comparable to the general population (non-carrier group) for those with ATM, CHEK2, and PALB2 mutations in the low risk PRS group (BOX 2), and it was noteworthy that about 30-40% of ATM and CHEK2 mutation carriers who did not have a family of breast cancer fell below the 20% risk threshold to justify, for example, enhanced screening measures such as breast MRI. Dr Isaacs noted that tools such as the PRS score, as they gain further validation, will be useful to facilitate individual decision making with patients to determine which management and/or preventive strategies are best for them. She also noted that, while guidelines such as those of the National Comprehensive Cancer Network (NCCN) are useful to inform on management for patients with more moderate penetrance genes such as ATM and CHEK2, such guidelines are constantly being modified and amended, so it is essential to check for the latest updates before counseling patients.
Box 2 – Breast Cancer Risk by Age 80 in those having No Family History of Breast Cancer According to PRS Group (Low or High)
| Mutation |
10th Percentile (Low Risk PRS) |
90th Percentile (High Risk PRS) |
|---|---|---|
| None (non-Carrier) | 6.7% | 18.3% |
| BRCA 1 | 36.1% | 46.9% |
| BRCA 2 | 43.8% | 49.5% |
| ATM | 12.8% | 32.3% |
| CHEK2 | 15.2% | 37.3% |
| PALB2 | 21.5% | 49.2% |
Results based on ~26,000 breast cancer cases and ~26,000 controls with testing for pathogenic variants and PRS score (105 common variants).
Contralateral Breast Cancer (CBC)
In patients who have a germline mutation in one of the breast cancer-associated genes who have already developed breast cancer, a prophylactic mastectomy of the other non-affected (i.e., contralateral) breast can be considered. BOX 3 shows the 10-year risk for a contralateral breast cancer for patients with breast cancer having a mutation in the BRCA genes, PALB2, ATM, and CHEK2, as reported in the CARRIERS Study.
Box 3. Cumulative 10-Year Risk for Contralateral Breast Cancer (CBC) in the CARRIERS Study
| Gene | 10-Year CBC Risk |
|---|---|
| Non-Carrier (No mutation) | 4% |
| BRCA1 | 23% |
| BRCA2 | 17% |
| PALB2 | 8% |
| ATM | 4% |
| CHEK2 (All pathogenic variants) | 8% |
| CHEK2 c.1100delC | 8% |
Dr Isaacs also noted that age at diagnosis for the primary breast tumor can impact CBC risk for selected moderate penetrance genes; for example CBC risk was markedly increased for premenopausal versus postmenopausal womenin the case of BRCA1, BRCA2, CHEK2 and PALB2 (BOX 4). Similarly, hormone receptor status has also been shown to impact CBC risk; for example, estrogen receptor (ER) negative status increases risk in non-carriers, BRCA1, and especially PALB2 patients, whereas those with ER positive status and ATM or CHEK2 mutations had a higher risk of CBC in one study.
Box 4. Impact of Age and Hormone Receptor Status on 20-Year CBC Risk
| Gene |
Premenopausal |
Postmenopausal |
ER+ |
ER- |
|---|---|---|---|---|
| Non-Carrier | 5.8 | 3.7 | 3.8 | 5.4 |
| BRCA1 | 33.4 | 11.5 | 17.1 | 27.7 |
| BRCA2 | 27.2 | 9.4 | 16.9 | 14.6 |
| ATM | 2.9 | 4.6 | 4 | - |
| CHEK2 | 13.2 | 4.3 | 8.2 | - |
| PALB2 | 12.2 | 5.1 | 1.9 | 19.7 |
Dr Isaacs also reviewed data for the BRCA contralateral risk (BRCA-CRisk) prediction model for patients with BRCA gene mutations. This model showed a number of clinical factors to be significantly predictive of CBC risk, including a younger age at first diagnosis of breast cancer (P=0.002), a first degree relative with either breast or ovarian cancer (P=0.011), a pathogenic variant of BRCA that is located in a specific (3’end) region within the gene (P=0.006) and the use of endocrine therapy versus not receiving therapy (P=0.013). While this model is not yet ready to be used clinically, some examples of how incorporating these clinical factors can affect risk for BRCA carriers is shown in BOX 5
Box 5. How Do Clinical Parameters Impact CBC Risk in BRCA Carriers?
| Age | Family History | Endocrine Therapy? | Mutation | 10 year CBC Risk |
|---|---|---|---|---|
| 38 Years | No | Yes | gBRCA2 (not 3’end) | 5.5% |
| 55 Years | Yes | No |
gBRCA1 (near 3’end) |
56.0% |
Impact of Bilateral Mastectomy
As noted above, prophylactic contralateral mastectomy is a consideration for patients with a primary breast tumor who have an increased genetic risk, and in this regard, Dr Isaacs reviewed data from an international cohort study of nearly 2500 women with gBRCA mutation, examining the impact of unilateral (one breast) or bilateral (both breasts) mastectomy versus breast conserving surgery (BCS, i.e., removal of just the tumor) in gBRCA patients. The results showed that the risk of developing a CBC was 10.8% for patients undergoing BCT versus 11.4% with unilateral and (as would be expected), nearly zero (0.8%) with a bilateral mastectomy. There was not, however, a significant difference in breast cancer related mortality for those undergoing a bilateral mastectomy as compared with BCS.
Who Should Be Tested?
In the final portion of her presentation, Dr Isaacs highlighted that the current recommendations for genetic testing in individuals with breast cancer have changed, based on a recent update by the American Society of Clinical Oncology (ASCO). Dr Isaacs also noted the current indications for BRCA gene testing (BOX 6), which includes all newly diagnosed patients of age 65 or younger, selected patients age 65 or older (e.g., TNBCs, Ashkenazi Jewish ancestry), and those with family or personal breast cancer history. Testing for other high or moderate penetrance genes (e.g., PALB2) could also be considered for such patients. The guidelines also stress that individuals found to have mutations whose overall impact on breast cancer risk is not known (termed a “variant of uncertain significance” or ‘VUS’) should not not alter their disease management course (i.e., should not be managed as if they had a true mutation). As more information on the given VUS is obtained, however, further follow up or evaluation might be indicated, so again it is important to check for any relevant updates that might impact the patient’s care. Dr Isaacs further noted that any patient who met the current criteria at the time of their breast cancer diagnosis and were not offered genetic testing previously should be offered such testing today to better understand their risk and any implications it might have for management.
Box 6 – Current ASCO Recommendations for BRCA 1 and 2 Testing
BRCA 1/2 Testing Should Be Offered to:
All newly diagnosed breast cancer patients < 65 years of age
Selected patients > 65, including those with TNBC, male breast cancer, Ashkenazi Jewish descent, those with multiple primary breast cancers, those with metastatic disease, and certain patients having gastric cancers or a family history thereof.
Those with a history of breast cancer who meet the above criteria.
Consider testing for moderate penetrance genes as well.
VUS should not alter treatment plan, but may need to be reassessed as new information emerges.
Speaker Disclosure Information: Dr Isaacs reported the following disclosures for this presentation: Consultancies: AstraZeneca, Biotheranostics; Genentech, Gilead, ION, Merck, MJH Holdings, Novartis, Pfizer, PUMA, Seagen; Royalties: Wolters Kluwer (UptoDate); McGraw Hill (Goodman and Gillman); Research Support (To institution): Tesaro/GSK; Seattle Genetics; Pfizer; AZ; BMS; Genentech; Novartis; Regeneron.
You can see the full presentation from the 2024 University of Kansas Breast Cancer Year in Review here:
Related Resources